Our Services
| Cleft lip/palate clinic | ||
|---|---|---|
Cleft lip/palate clinic
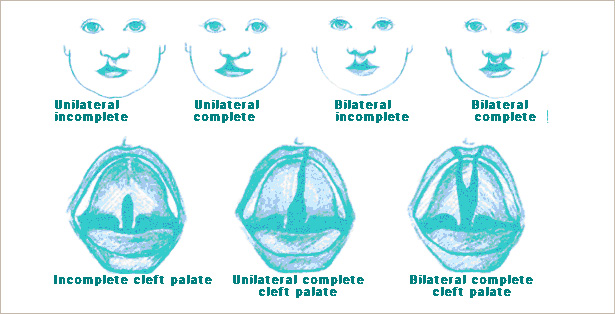
What is cleft?Cleft is congenital separation of lip and/or the palate. Sometimes alveolus and maxillary bone are also involved. Congenital separation of the lip is called 'cleft lip', and that of the palate is 'cleft palate'. 'Alveolar cleft' implies the separation of the alveolus. Actually baby has little discomfort with this condition. This congenital anomaly is known to appear in 1st trimester. Etiology is thought to be the genetic and environmental factors. Therefore, no parents should be blamed or feel guilty. Incidence is different among the ethnic group, about 1 of 700~750 babies have this condition when he or she is born
What can we do to manage the cleft baby?Special care should be taken to the cleft baby from the birth. Although there is individual difference, several times of admission and surgery are necessary. We’ll show you the sequential management of this cleft baby.
What can we do to manage the cleft baby?~1 year old : When they are born, consultation to the pediatric specialist about the genetic counseling and breast feeding should be preceded. Around the age of 10 weeks, cheiloplasty is planned. The purpose of this surgery is attaching the separated lip with minimal scar and improving the aesthectic and functional growth. At the same time, primary rhinoplasty to restore the normalized shape of the cleft side nose. In case of cleft palate, palatoplasty should be planned around the 11 months. With the cleft palate, they tend to have otitis media due to the disturbed muscle function. Therefore, consultation to the ENT specialist should be preceded around 6 months and simultaneous tube insertion must be considered. Most of the cleft palate patients have normal pronunciation, however they have possible tendency of slowed speech development and articulation problem, therefore co-work with speech therapist should be started around 3 ~ 6 months of age and follow-up should be made every 6 ~ 12 months.
Breast feeding and postoperative care of clef lip / palateParents get to know that there is little difference in breast feeding between the cleft and the non-cleft baby though they are somewhat embarrassed at first. Cleft baby need same amount of the caloric uptake and nutritional support. Cleft baby has weak suckling power due to the cleft lip and/or palate, therefore the food tends to regurgitate over the nose. They are easily tired before the completion of the lactation because of this difficulty in sucking. In fact, it is very hard for the cleft baby to suckle via the nursing bottle. Therefore, cruciform hole on the nipple and squeezing a little during the breast feeding may be needed to help the cleft baby. It is recommended that breast feeding should not last more than 30 minutes. As they swallow air during the lactation, parents should make them belching intermittently. They have a tendency of sneezing and swallowing the wrong way, so they should be orthostatic in some degree during the milk feeding and with the slower rate than the non-cleft baby.
Issue of health insurancePrimary cases of cleft lip and palate are covered with health insurance. However, all other cases except the primary cases are beyond the coverage of health insurance. For financial support or more information, call 02-3101-4090, department of public welfare service in Asan foundation.
Postoperative careFollowing the palatoplasty, cleft baby should be in the prone position so that the intraoral bleeding should not be aspirated and discharged naturally. Immediately after the surgery, some bleeding is natural and parents don’t have to be worried about this. It is important for the cleft baby to leave the intraoral suture untouched. They should not put their hands into the mouth or suck their finger. If needed, restriction of the hands may be needed. Crying may cause the tension to the suture site and may result in the wound dehiscence so the parents should make them calm down and asleep. Although breast feeding is possible from the day after the surgery, syringe or spoon is recommended other than the nurse bottle nipple. After the milk feeding, water intake should be followed to remove the remainder of the milk on the suture site. Though stitches disappear in 2 to 3 weeks spontaneously, special care should be taken until this period and parents should not make them cry.
Development of the teethCleft lip / palate patient has different teeth structure from that of non-cleft patient. Lack of the number of teeth or excess of the number of useless teeth is not infrequent. Shape of the tooth adjacent to the alveolar cleft is unusual and crooked. Dental specialist for the cleft paitent may help this patient with the specillay designed orthodontic treatment.
Secondary deformity of cleft lip and noseClef lip patient has typical structural deformity of nose. In case of unilateral cleft, nose is deviated to the non-cleft side, ala of cleft side is drooped and depressed, nostril of cleft side is widely opened, and nasal floor of the cleft side is depressed so that the apparent asymmetricity is prominent. Surgery for this deformity is planned at preschool age; 1 to 1 and half year before admission. Adequate timing of definite corrective rhinoplasty had better be postponed until the growth of bone and cartilage is completed. This is planned after the adolescent period. Secondary cheilorevision is planned with the secondary rhinoplasty. However, if the scar around the philtrum is widened abnormally, line of lip is severely interrupted, notching or bulging of vermilion is prominent, cheilorevision can be planned at appropriate time.
|
||