Eyelid Surgery
Double eyelid surgery
From old times, eye is called 'window of the heart' and is regarded as the most important decisive part that make one's first impression. Double eyelid surgery is to place a pretarsal crease in Asian eyes that are absent from the fold. Patients may complain of difficulty in applying eyeliner because of the overhanging fat. Patients typically desire to look more bright-eyed and want to make applying eyeliner easier. Patients also seek to remove the puffy and tired look associated with a fatty upper lid. Most of the Korean people don't have the double eyelid and have bulging and swollen eyelid. Double eyelid surgery can make clearer impression.
Surgical indications
Double eyelid surgery is indicated for the patient who has no double eyelid at all or one side only. Patients with bulging and swollen eyelid or with thick fatty layer can get rid of fat simultaneously. Patients with ptosis or hooding of eyelid can take excision of eyelid wrinkle and make double eyelid. However, appropriate procedure should be dependent on the individual characteristic. On occasion, there are patients who should not take double eyelid surgery, so it is necessary for the patient to get thorough consultation to the plastic surgeon.
Preoperative preparation
To prevent the bleeding or hematoma, NSAID including aspirin had better be avoided before surgery. On the day of surgery, it is recommended to bring sunglass to wear after the surgery.
Surgical procedures
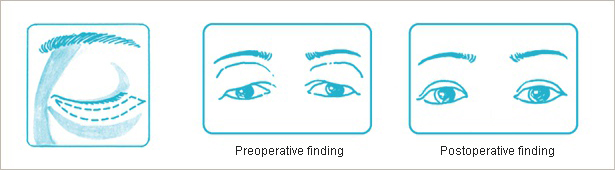
Double eyelid surgery is performed under the local anesthesia and anxiolytics may be added if necessary. There are two ways of double eyelid surgery. One is 'Incisional approach' and the other is 'Buried Suture Method'. Incisional approach includes the skin incision of the eyelid and partial excision of muscle and skin leading to the double eyelid line. Fat tissue can be gotten rid of if it is necessary but scar may be visible along the incision lines. However, it doesn’t matter too much because this scar gets vague and it can be hidden by the double eyelid fold. Patients with thin eyelid skin and scanty fatty layer is the best candidate for the 'Buried Suture Method' as scar is almost invisible and natural fold can be obtained. However, double fold gets loose from time to time.
Postoperative care
Postoperative pain can be managed by the analgesics. For 2 to 3 days after the surgery, head elevation and ice massage are recommended to reduce the swelling. Stitch out can be made in 3rd to 4th day after the surgery and make-up is possible the day after stitch out.
Return to the normal daily life can be ensured in 1 week, but stable double eyelid fold is placed in 2 to 3 months. It looks unnatural immediately after the surgery due to the swelling and bruise. However it gets better as time goes by.
Blepharoplasty
Blepharoplasty is the procedure that removes the redundant skin of upper and lower eyelid and bulging of lower eyelid and sometimes corrects the ptotic upper eyelid. Prominent fold of upper and lower eyelid and sagging of lower eyelid make one look tired and older for their age and visual disturbance. Blepharoplasty can improve these functional problems as well as the cosmetic concerns.
Indications
If the fold of upper and lower eyelid is too deep, festered lateral upper eyelid due to the hooding, bulged under the lower eyelid causing the senile and tired appearance, surgical intervention may work. After counseling and physical examination, whether the surgery is indicated or not is determined. Upper and lower blepharoplasty can be performed in one or two separate stages.
Preoperative preparation
Most of all general examination for the eye should be made. The patient should be given sufficient explanation about the postoperative outcome and possible complications. Smoking and NSAID including aspirin should be forbidden for 2 weeks before surgery. On the day of surgery, it is recommended to bring sunglass to wear after the surgery.
Upper blepharoplasty
 Upper eyelid is one of the first sites that senile change is noticed. The reason is that the skin of upper eyelid is thinner than all other part of the body and has thin fatty layer as well. As periorbital muscles are most commonly used in daily life, this is another reason for aging of upper eyelid. With this senile change deepened fold and wrinkle as well as visual disturbance and trichiasis often develop.
Upper eyelid is one of the first sites that senile change is noticed. The reason is that the skin of upper eyelid is thinner than all other part of the body and has thin fatty layer as well. As periorbital muscles are most commonly used in daily life, this is another reason for aging of upper eyelid. With this senile change deepened fold and wrinkle as well as visual disturbance and trichiasis often develop.
Upper blepharoplasty includes the correction of sagging and drooping of upper eyelid and bulging of fatty tissue. Incision is designed along the natural eyelid fold and removal of the skin, muscle, and fatty layer is planned as needed.
 Refined diagnosis should be preceded because the clinical manifestations show extremely various spectrums with individual difference. The patient may have sagging of the eyelid with the drooping of skin only, sagging eyelid accompanying the muscle hanging, bulging with excessive fatty tissue. If the sagging of the upper eyelid is caused by the ptosis, correction of ptosis should be performed together. Most of the surgery can be made under the local anesthesia and stitch out is planned around the postoperative 4th day. After 1 week, daily activity and social life can be resumed. Preoperative counseling is necessary if the patient takes anticoagulant agent or has hig blood pressure because the convalescent period may be longer in this case.
Refined diagnosis should be preceded because the clinical manifestations show extremely various spectrums with individual difference. The patient may have sagging of the eyelid with the drooping of skin only, sagging eyelid accompanying the muscle hanging, bulging with excessive fatty tissue. If the sagging of the upper eyelid is caused by the ptosis, correction of ptosis should be performed together. Most of the surgery can be made under the local anesthesia and stitch out is planned around the postoperative 4th day. After 1 week, daily activity and social life can be resumed. Preoperative counseling is necessary if the patient takes anticoagulant agent or has hig blood pressure because the convalescent period may be longer in this case.
Lower blepharoplasty
As one grows old, skin of lower eyelid gets thin, tension of the muscle is decreased, orbital septum becomes weaker and orbital fat is protruded so that the bulging of fat in the lower eyelid is prominent. Over time, predisposed individuals develop attenuation of the orbicularis oculi muscle and laxity of the attachments between the orbicularis and the deep fascia. The orbicularis progressively sags until folds of muscle are suspended across the lid, emulating gathered bunting. Some patients cite a history of familial occurrence of these folds. This phenomenon can affect any part of the upper or lower eyelid. However, the unmodified word festoon, without anatomic specification, has come to refer most often to sagging of the orbital and malar segments of the orbicularis oculi muscle of the lower eyelid.
Commonly, protruding intraorbital fat and septum accompany festoons; however, occasionally, festoons are composed solely of muscle and skin. Corrective surgical steps are directed at tightening the slack muscle and skin.
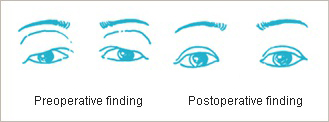
Through blepharoplasty, partial removal of protruded orbital fat and redistribution can be achieved and laxity of orbital septum is tightened and skin and muslc sagging is corrected.
If there is only the festoon without skin laxity or muscle sagging, transconjunctival incision without external skin incision is preferred. On the contrary, too much depressed eyelid can be helped with fat graft to be rejuvenated.
Postoperative finding
Postoperative care
In most of the cases, postoperative pain can be handled with analgesics. Head elevation for 2 to 3 days after the surgery with ice massage is recommended. The patient had better be told that they should avoid watching TV on lying position or reading a book for a long time. Stitch out can be completed within 4 to 5 days after the surgery. One day after stitch out, the patient can make up. The patient can go back to their daily life in 1 week though the periorbital swelling and bruise may last for 2 to 3 weeks. Temporary tearing and dazzling may occur, which is spontaneously resolved.
Blepharoptosis
Most of all general examination for the eye should be made. The patient should be given sufficient explanation about the postoperative outcome and possible complications. Smoking and NSAID including aspirin should be forbidden for 2 weeks before surgery. On the day of surgery, it is recommended to bring sunglass to wear after the surgery.
Preoperative preparation
 Blepharoptosis is a downward placement of the upper eyelid margin in relation with the superior limbus of the cornea. In general, upper eyelid covers 1 to 2 mm of the superior limbus. If the upper eyelid under the influence of blepharoptosis droops to cover the upper limbus or pupil, surgical intervention may be indicated.
Blepharoptosis is a downward placement of the upper eyelid margin in relation with the superior limbus of the cornea. In general, upper eyelid covers 1 to 2 mm of the superior limbus. If the upper eyelid under the influence of blepharoptosis droops to cover the upper limbus or pupil, surgical intervention may be indicated.
Patients with blepharoptosis tend to glare for opening the eye with help of forehead, which results in wrinkles on the forehead and raising the jaw upward inconsciously. In severe cases, amblyopia may be accompanied because the affected eye is out of use.
Etiology
Blepharoptosis is generally classified into the congenital and acquired type.
Congenital ptosis includes isolated myogenic type leading to the poor development of levator muscle with functional deficit and neurogenic type like Marcus-Gunn pupil and cranial nerve III palsy. It can involve unilateral or bilateral eyelids. Patients with congenital ptosis cannot open their eyes immediately after the birth. With the age of controlling their neck, patients have a tendency of raising their neck and jaw.
Acquired ptosis includes mechanical, traumatic, neurogenic, and senile types. Causes of mechanical ptosis include tumor, cyst, and structural deformity like enlarged lacrimal gland. Traumatic ptosis presents various symptoms according to its site of injury, remaining levator muscle function and eyelid opening mechanism. Neurogenic ptosis is caused by the acquired CN III palsy, myasthenia gravis, and Horner’s syndrome. In senile ptosis, thinning and lengthening of levator muscle or disinserted levator aponeurosis from the tarsal plate can be observed. Therefore, blepharoplasty with correction of blepharoptosis should always be considered in patients with senile ptosis.
Treatment
In case of congenital ptosis, surgical intervention is planned at the age of 3 to 5 years. Patients with congenital ptosis have little visual acuity immediately after the birth. Power of vision grows with using the eye. However, this visional development is limited and amblyopia may occur. To prevent this amblyopia, correction of blepharoptosis is mandatory when the patient is 3 to 5 years old. In severe blepharoptosis, other procedure to prevent the amblyopia should be considered even before age of 3 to help visual power growth. For the baby with congenital blepharoptosis in age of 2 to 3 months, bandage can be used to lift the eyelid and fixed on the forehead. In some cases, blindfold is applied on the unaffected side so that the affected side is forced to be used. If the underdevelopment of the visual power in the affected side despite of these trials lasts, early surgical intervention is indicated.
Surgical techniques
Surgical techniques are selected based on the etiology, degree of ptosis, and remaining levator function. For the correction of congenital blepharoptosis, levator placation-shortening or advancement technique is preferred. For the correction of mechanical ptosis resulting from the tumor or cyst can be handled with removal of the mass itself. In case of traumatic ptosis, reinsertion of the levator muscle or the levator aponeurosis and the Müller muscle to the tarsal plate. With the patients with paralytic posttraumatic blepharoptosis, wait until the recovery of the nerve imporves the symptoms then levator placation could ensue. If the nerve never restores, frontalis sling to the tarsal margin can be considered. Shortening of aponeurosis and reinsertion into the upper border of the tarsal plate improve the symptoms in case of involutional blepharoptosis.
Complications
The most common complication is incomplete correction. Other complications include lagophthalmos, asymmetric correction, irritation, and contour deformity.
Overcorrection can result in the lagophthalmos and asymmetric appearance. In case of lagophthalmos, corneal erosion or ulceration due to the longstanding exposure can threaten the visual acuity. Therefore it is crucial to protect the cornea with artificial tears, ophthalmic ointment, and forced eyelid closure by taping.
If scar adhesion disturbs the eyelid motion and induces lagophthalmos, adhesiolysis is indicated.
Thorough control of bleeding cannot be emphasized too much in eyelid surgery. Acute hemorrhagic complication may threaten the visual acuity and even result in catastrophic blindness.
Temporary or persistent complications relevant to the correction of blepharoptosis are visual disturbance, corneal erosion, ulceration, and abrasion, destruction of periorbital apparatus including eyelashes, chemosis, and diplopia. Among these complications, chemosis occurs not infrequently, however it subsides with expectation.